MESENCHYMAL STEM CELLS: A Curative Treatment for Psoriasis
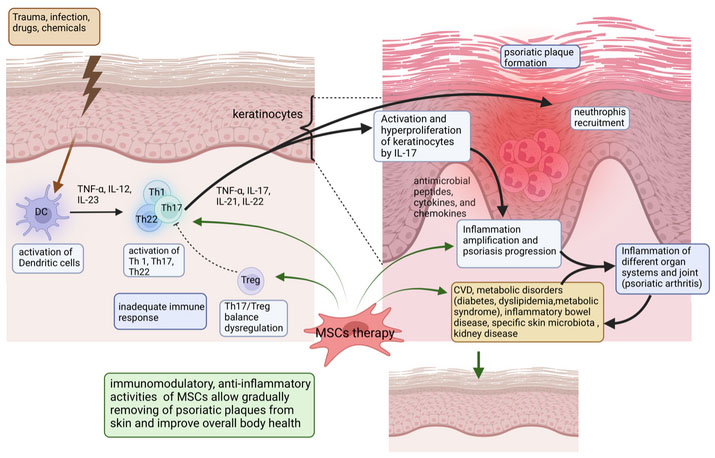
Psoriasis is a chronic immune-mediated systemic disorder induced by multiple environmental factors. These environmental factors such as infection, stress, or trauma activate cutaneous dendritic cells to produce tumor necrosis factor (TNF)-α and interleukin (IL)-23, which subsequently stimulate the proliferation and differentiation of proinflammatory T- lymphocytes cells. Tregs are a subpopulation of regulatory T lymphocytes that could suppress the excessive immune response and maintain immune homeostasis. There is also another subpopulation of T lymphocytes that release cytokines to help other immune cells generate appropriate responses to different pathogens (e.g. viruses, bacteria).
Generally, the pathogenesis of psoriasis for genetically predisposed individuals starts with the overactivation of Th1, Th2, and Th17 cells, which leads to an impaired balance between Treg and Th cells, and an excessive elevation levels of proinflammatory cytokines. Th17 expressing IL-17 induces keratinocyte proliferation up to 10 times faster than normal. This led to forming bumpy red patches covered with white scales, which appear on the scalp, elbows, knees, and lower back. In addition, approximately 10% to 30% of individuals with psoriasis also developed psoriatic arthritis, causing pain and swelling in the joints.
To date, a variety of treatments used for psoriasis aim to reduce symptoms of the disease, to stop skin cells from quickly amplifying, and to remove scales. The selected therapy option for a patient depends on the severity of the disease manifestation and includes creams and ointments (topical therapy), light therapy (phototherapy), and a variety types of medications that could be administered orally or intravenously. Immunological and genetic studies have identified that activation signals from the IL-17 and IL-23 could be a key driver of psoriasis pathogenesis. Biologic drugs targeting TNF-α, IL-17, and IL-23 have been developed and achieved significant clinical outcomes. In spite of that, these agents can cause serious side effects and are prescribed for advanced disease cases. There could be a necessity to try different drugs or a combination of treatments before finding a working variant for each particular case. But even with successful treatment options, psoriasis symptoms return in most cases.
Currently, mesenchymal stem cells (MSCs) therapy appears to be a safer therapeutic approach for advanced psoriasis patients. These cells are naturally occurring in the body but are very rare compared with many other cell types. During the MSCs therapy, patients will get locally and intravenously booster doses of these cells.
MSCs are characterized by regenerative abilities and immunomodulatory properties, and are often used in recovery medicine. It is well established that MSCs possess immunomodulatory functions on T cells, B cells, and other innate immune cells, mainly through paracrine mechanisms by secreting extracellular vesicles and cytokines, or by direct cell-to-cell interaction. The investigation of MSCs mechanism of action for psoriasis patients showed that therapeutic effects are achieved due to regulating the balance of Th1, Th2, Th17, and Treg responses by secretion of PGE2 and TGF-β molecules. Some studies suggest that MSCs infusions may promote T-cell differentiation into Tregs and memory T cells.
Moreover, there are several clinical trials and case reports of MSCs treatment for psoriasis patients which showed great therapeutic effects. For example, Xiangya Hospital Central South University in China performed a single-center, open-label, single-arm clinical trial for 17 patients with psoriasis (registration number: NCT03765957).
After the sixth month of therapy, 47.1% (8/17) had at least 40% improvement, 35.3% (6/17) had more than 75% improvement and 17.6% (3/17) had more than 90% improvement according to the PASI score. There were no serious adverse events, major abnormalities in clinical analysis, or biochemical indices for the heart, liver, and kidney function; and there were no infection complications or cancer observed associated with MSCs therapy. As a result, MSCs could outperform the convenient immunosuppressive biological drugs for psoriasis treatment in terms of safety for health.
Having said that, there were a few cases of disease relapse 8-12 months after MSCs administration. This recurrence may be explained by the limited duration of MSCs immunomodulatory effects and the persistence of pathogenic factors causing disease manifestation. Thus, a repeated MSCs infusion is necessary after several months to avoid disease relapse.
MSCs such as Kintaro cells have great immunomodulatory and other therapeutic properties characteristic for MSCs. Kintaro Cells are bone marrow-derived obtained from young, healthy donors and Kintaro Cells Power has a rich experience in treating various disorders, including psoriasis.
Sources:
- https://www.nature.com/articles/s41392-022-01059-y
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7142341/
- https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8362539/#!po=17.5676
- https://www.mayoclinic.org/diseases-conditions/psoriasis/diagnosis-treatment/drc-20355845
- https://www.psoriasis.org/treatments-for-psoriatic-disease/